BENEFITS CENTER
Dental Benefits
Compare the available Platinum Control dental benefit options below.
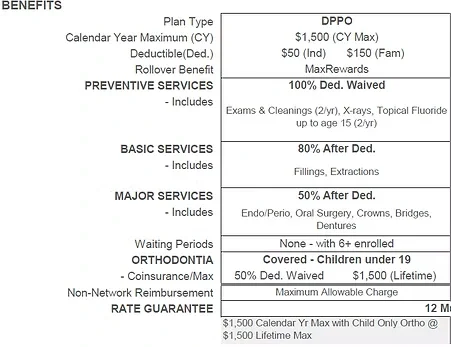
OPTION 1
Base Plan
PROVIDER
Ameritas — Co-Ins MAB Classic 1500
WAITING PERIOD
1st of month following 30 days
COST BREAKDOWN
Employee Only
Per Paycheck $0.00
TOTAL / YR EMPLOYER EMPLOYER
$384.80 $384.80 $0.00
Employee + Child(ren)
Per Paycheck $15.59
TOTAL / YR EMPLOYER EMPLOYER
$805.22 $384.80 $420.42
Employee + Spouse
Per Paycheck $14.81
TOTAL / YR EMPLOYER EMPLOYER
$769.86 $384.80 $385.06
Employee + Family
Per Paycheck $31.31
TOTAL / YR EMPLOYER EMPLOYER
$1,229.28 $384.80 $844.48
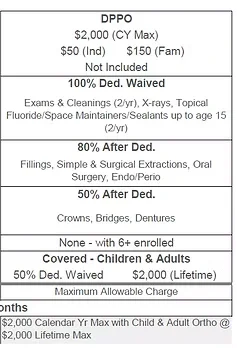
COVERAGE INFORMATION
OPTION 2
High Deductible PPO Plan
PROVIDER
Ameritas — Co-Ins MAB Classic 200
WAITING PERIOD
1st of month following 30 days
Employee Only
Per Paycheck $7.63
TOTAL / YR EMPLOYER EMPLOYER
$583.18 $384.80 $198.38
COST BREAKDOWN
Employee + Child(ren)
Per Paycheck $32.13
TOTAL / YR EMPLOYER EMPLOYER
$1,220.18 $384.80 $835.38
Employee + Spouse
Per Paycheck $30.05
TOTAL / YR EMPLOYER EMPLOYER
$1,166.10 $384.80 $781.30
Employee + Family
Per Paycheck $56.84
TOTAL / YR EMPLOYER EMPLOYER
$1,862.64 $384.80 $1,477.84
COVERAGE INFORMATION